

Quality Within Critical Access Hospitals: The Benefits and Challenges of Tracking Measures
Although Critical Access Hospitals have largely been exempt from quality measure reporting, they are required to maintain a quality program and submit their data to at least one quality improvement organization or state agency. As a Condition of Participation (COP), a CAH must develop and maintain a hospital-wide quality assessment and performance improvement (QAPI) program. This program must include all departments of the hospital, including those with contracted providers and it must address health outcome measures.
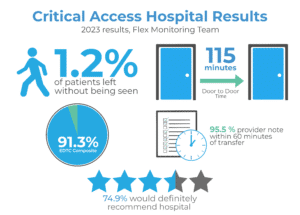
Many CAHs voluntarily participate in The Medicare Beneficiary Quality Improvement Project (MBQIP), which focuses on quality improvement within the Medicare Rural Hospital Flexibility (Flex) Program. Hospitals that commit to participating in MBQIP are able to apply for a multitude of different grants and training programs through their state’s Flex program. As of 2023, 95.5% of CAHs submitted at least one measure to the Flex program [1].
There are three MBQIP measures for 2026 that focus specifically on the emergency department:
- Emergency Department Transfer Communication: The percentage of patients who are transferred from the ED to another facility that have all necessary communication made available to the receiving facility in a timely manner
- Door to Door Time: ED arrival to discharge. This measure excludes patients that are admitted, transferred, transpired or that left AMA.
- Left Without Being Seen: Percentage of patients who left the ED prior to being evaluated by a provider.
In addition to MBQIP measures, patient experience scores are an important part of any QAPI program. Integrating patient satisfaction scores allows hospitals to identify gaps that might otherwise not be identified, such as communication issues or comfort level of the hospital and patient rooms. The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey is a required element for the MBQIP and Flex programs; this is a patient experience survey that is administered by CMS approved third-parties to hospital inpatients. A minimum of 100 responses must be received for the scores to show on the CMS Care Compare website. To capture patient experience scores for outpatient services, including ED patients, many hospitals use the CMS approved ED-CAHPS survey. These surveys are not mandatory. Although the sample size of returned surveys is often low for CAHs, they can nonetheless provide actionable insight for quality improvement initiatives.
Why Is This Important to Hospitals and Providers?
- Studies show 25% of ER patients have inadequate health literacy, meaning they have difficulty participating in medical decisions, following medical recommendations and attending follow-up appointments. Better provider-patient communication helps avoid post-discharge adverse events and readmission. [2].
- Physicians with more than 2 patient complaints a quarter were 4 times more likely to have a risk management episode (defined as formal case review or malpractice lawsuit). [3]
- A longer length of stay in the ED may indicate inefficiencies within the department and/or its supporting services, increasing the risk of adverse patient outcomes and potentially leading patients to avoid that ED in the future. [4]
- Patients that leave without being seen by a physician represent a quality concern to CMS; up to 25% of these patients return to an ED within 7 days, and 11.5% of these patients are subsequently admitted. While patients that LWBS represent a revenue loss for hospitals initially, those that return often have high acuity symptoms that require a higher tertiary level of care. [5].
- Most CAHs have Medicare Star ratings published for at least one measure. These allow patients to evaluate a hospital prior to coming in for care. These also allow Medicare Advantage plans to evaluate their network and negotiated rates with hospitals; MA plans don’t reimburse CAHs on a cost basis like traditional Medicare.
Challenges with Patient Experience Surveys
- Most patient experience surveys, including HCAHPs and Press Ganey, cannot give provider-specific feedback for hospital units; instead, patient feedback is attributed to the attending physician at discharge.
- These surveys exclude patients that are discharged to hospice care or nursing homes; these patients often require a lot of the provider’s attention and yet their feedback is not solicited.
- For ED surveys, patients that are admitted to the hospital will not receive ED specific surveys and will instead be part of the eligible pool of patients to receive inpatient surveys. This can skew ED patient satisfaction results to focus on the less acute patients that may have had longer wait times due to triaging protocols.
- Patients that are transferred will not receive a survey; this can make it harder for smaller hospitals to achieve an appropriate sample size.
STATUS is a full-service physician practice management company that has been in business for over 30 years. STATUS is physician owned and physician led. In addition to provider staffing, STATUS has an experienced quality management team that assists with hospital-wide quality initiatives.
- Lahr, M., Furukawa, A., Pick, M., & Barclay, R. (2025). MBQIP quality measures national annual report: 2023. Flex Monitoring Team, University of Minnesota. https://www.flexmonitoring.org/sites/flexmonitoring.umn.edu/files/media/MBQIP_quality_measures_national_annual_report_2023.pdf
- Shahid, R., Shoker, M., Chu, L.M. et al. Impact of low health literacy on patients’ health outcomes: a multicenter cohort study. BMC Health Serv Res 22, 1148 (2022). https://doi.org/10.1186/s12913-022-08527-9
- Jacques, T. S., & Sebire, N. J. (2010). The impact of article titles on citation hits: An analysis of general and specialist medical journals. JRSM Short Reports, 1(1), 2. https://doi.org/10.1258/shorts.2009.100020
- Ortíz-Barrios, M. A., & Alfaro-Saíz, J.-J. (2020). Methodological Approaches to Support Process Improvement in Emergency Departments: A Systematic Review. International Journal of Environmental Research and Public Health, 17(8), 2664. https://doi.org/10.3390/ijerph17082664
- Li, D. R., Brennan, J. J., Kreshak, A. A., Castillo, E. M., & Vilke, G. M. (2019). Patients Who Leave the Emergency Department Without Being Seen and Their Follow-Up Behavior: A Retrospective Descriptive Analysis. The Journal of emergency medicine, 57(1), 106–113. https://doi.org/10.1016/j.jemermed.2019.03.051